That a well known oncologist, who earlier in the day had given a fascinating scientific presentation, taught us some Bollywood moves at the final dinner gives you a little bit of a feel for what this conference was like. (Link below is to a video of us doing our best to Sapphire, the song by Ed Sheeran and Arijit Singh).
https://mylivercancerblog.com/wp-content/uploads/2026/05/img_6916-1.mov
The conference brings together world class researchers, most of whom are also clinicians, with patients, caregivers, and even some representatives from the drug manufacturing industry. Most of the presentations are pitched at a clinician/researcher level, but with enough layperson scaffolding and take-home points to make them fairly accessible to patients. Accessible enough to be really interesting. And much of the research is truly cutting-edge, with the presenters noting that the data is “in press” or “not yet published.”
And everyday there were also presentations by patients, all of which were moving. There was a patient from New Zealand who talked about what it was like to be diagnosed and not be able to find online a single other person in the country who had the disease. And so she started a group for patients, put together educational materials, contacted oncologists all over the country, reached out to every new patient she could find. She didn’t want anyone to go through what she had — feeling so alone in her diagnosis that she sometimes wondered if she had made it all up. There was also an infuriating and inspiring talk by Keaton Herzer, whose liver transplant surgery was initially denied by his insurance company (the decision was eventually reversed, and he is now 30 days post-transplant and doing well). I feel a special kinship with Keaton because his tumours also had the NRG1 fusion mutation, and it was infusions with zenocutuzumab that shrunk his tumours enough to make him eligible for transplant surgery.
https://vt.tiktok.com/ZS9sFR6dF/
https://vt.tiktok.com/ZS9sLKnnd/
(Sorry for all the links. I have not been able to make the WordPress video embed function work. The above are videos by Keaton about his experience, but I don’t know if they will work if you don’t have TikTok).
I have never been to or even heard of a conference that brings patients and doctors together like this. There were “ask the expert” panels, where patients could ask questions about their own situations to a joint panel of oncologists, surgeons, and radiologists. There was a panel that was presented as a “tumour board” (which all cancer hospitals have), where the panel members were given a hypothetical case study and told to discuss it in the way that they would at their home institutions: “female, 60 y.o., intrahepatic cholangiocarcinoma, 10 cm tumour in segments 4 and 5, previous history of diabetes, imaging looks like this (imagine a CT scan on a PowerPoint slide). Okay, Dr. Smith, how would you proceed?” “Okay, Dr. Green, you are a radiologist, and you have heard what Dr. Smith would do first, would you proceed any differently?” And so on. There were presentations by young postdocs and residents, where they had to present their original research findings in 3 minutes and then answer probing questions by experts in their field.
And the foundation knows that some patients are not very mobile or not very well off, so they provide all meals during the conference, so that no one needs to go wandering in search of food in a city they don’t know. And, I’ve got to say, there is nothing like being able to sit down for lunch and dive directly into asking the stranger next to you where they are from, when they were diagnosed and what their diagnosis is, what treatments they have received and what worked or didn’t. These are kind, empathetic, no bullshit conversations, and everyone’s stories are the same and yet totally different. No one could pronounce the name of the disease when they first found out, almost everyone had initial symptoms of bad fatigue, and thought they would just get over it. But some people have actionable tumour mutations and some don’t, the ones who do may have different mutations, some of which have targeted therapies, but some don’t, and even the ones with the same mutations taking the same targeted therapies often have different results – e.g. some patients with the IDH1 mutation see their tumours shrink when on Tibsovo, some don’t see shrinkage but their tumours remain stable for years, and for some it stops working after 6 months.
There are people who were able to get surgery very early on and were NED (no evidence of disease) for years, but just a few months ago they’ve had a recurrence. There are people who are still NED, but they remain ever vigilant and come to the conference every year to stay connected with the community and stay on top of new research. There are people who have gone from one treatment to another, managing to keep themselves alive for 5 years or more (chemo, then second line chemo, then radiation, then targeted therapy, a couple rounds of histotripsy, a clinical trial with a new targeted therapy, and so on and so on). There are “legacy caregivers” who lost loved ones to this disease, but have have found purpose in serving as mentors to newly diagnosed patients. There are patients who may be (but maybe not) at the end of the line. They’ve exhausted all the treatments they can, they’ve been coming to the conference for years and made and lost friends in those years, and they know this might be the last time they come to this conference (but maybe not…). And there are first time attendees, like me, who are blown away by the warmth and generosity of the patients they meet, who feel they have met “their people,” and who hang on the word of every single presentation from 8am to 5pm because what they can understand of the science is incredibly absorbing and has (or will have, maybe years from now) clinical relevance.
I learned that the incidence of cholangiocarcinoma is very likely much higher than researchers, clinicians, and epidemiologists realized. For years everyone has been saying that there are 8 – 10,000 new cases each year in the USA. Turns out that it is more like 20 – 25,000, at least since 2019. And some of this increase may be due to changing diagnostic criteria and better reporting, but the research team who presented the findings are convinced that much of the increase is an actual increase in incidence, though they do not know why. And it’s being found in younger and younger people. I learned that tumours create “micro-environments” around them that can vary by mutation. IDH1 mutations, for example, create “immune deserts” around them (powerful imagery that scares the shit out of me), meaning that T-cells flee the area and so immunotherapy is less likely to be effective because there are fewer T-cells to recruit to the cause of killing the cancer. I learned that researchers are turning more to “basket trials,” in which instead of trying a new drug on just one cancer, they instead try the new drug on a range of different cancers where the participants’ tumours have the same mutation (e.g. the FGFR2 mutation has been found in breast, gastrointestinal, and cholangiocarcinoma tumours). This allows them to recruit more patients to their clinical trial, and if the drug is successful in all the different cancers, the drug manufacturers can pursue approval of their drug for all the cancers at the same time (which makes them happy) and more patients will have access to the drug (which makes patients and oncologists happy).
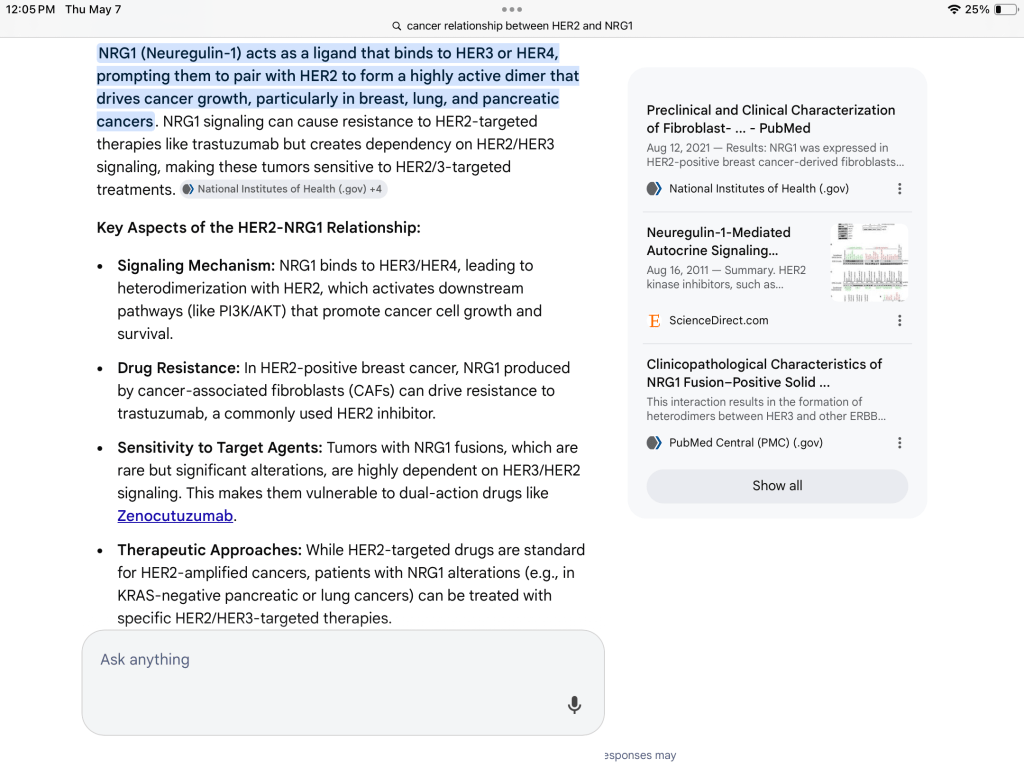
Interestingly, though a lot of the presentations would be categorized as falling into “precision oncology” and focused on research about specific tumour mutations, there was almost no mention of NRG1 fusion. There were a couple of scientific posters about zenocutuzumab’s efficacy in treating tumours with this mutation, and Keaton mentioned it in his talk, but there was little else. You could “build your badge” by sticking different things about you to it (e.g. first time attendee, IDH1, FGFR2, KRAS, caregiver, patient, etc.), but there was no NRG1 sticker I could affix to my badge. But then one researcher/clinician, almost in passing, mentioned that possibly zenocutuzumab might be effective for patients with the HER2 or HER3 mutations because the drug might possibly interrupt the pathway that leads to cell growth and division. There was no discussion of a clinical trial where this hypothesis might actually be tested. Below is what AI says about the relationship between NRG1 and HER2, but I don’t really understand it.
This post is already too long, so perhaps there will be a part 2 if I find things in my notes worth sharing. I’ll end by saying that the conference filled me with energy and hope. So many of the researchers said things like, “There have been more treatments discovered for this disease in the last 5 years than in the previous 20” and “cholangiocarcinoma is one of the most molecularly complex cancers there is (i.e. lots of different mutations), which can make it hard to treat, but also means that there are more opportunities for targeted therapies than for almost any other kind of cancer.” I really loved this conference, and I really hope I’m alive and well enough to go again next year.

Leave a comment