I received my first infusion of zenocutuzumab (Zeno) this week. It all went well — no side effects (knock on wood) except for some minor gastrointestinal upset — and this week I have felt fine. Better than fine, really — the closest I’ve felt to “normal” in a year. For example, yesterday I went for a 4 mile walk/run (including a short hill workout), did some grocery shopping, took the dogs to the park, and caught up on doing the dishes. It might not sound like much, but it’s more than I’ve done in one day in a very long time.

The most interesting thing about this experience so far is the clinic. It is a private infusion clinic, which is very rare in Canada. I didn’t know that such a thing existed here until my oncologist told me he was referring me to this one to receive the Zeno infusions. I think because the drug is not formally approved in Canada, it cannot be administered at the cancer hospital, or, for some reason I don’t understand, it would be too expensive to do so. From talking to the clinic owner, my impression was that any infusion that is off-label or not officially approved is done at private clinics, and most often patients are paying out of pocket. As he explained it, in the normal course of affairs, the cancer hospital provides treatment and then essentially submits receipts for reimbursement to Ontario Health. The finance people at Ontario Health scrutinize every receipt, and if the treatment doesn’t conform to the specifications permitted by them, they won’t provide reimbursement.
This means that not only are treatments like mine (an off-label use of a drug that isn’t approved in Canada) not covered, but also therapies that might be pretty standard are not covered if the treatment or the patient (their treatment history, for example) don’t match Ontario Health guidelines. So, for example, at the private clinic there was an older woman receiving durvalumab (immunotherapy). I’ve been receiving infusions of durvalumab at the cancer hospital for free for 9 months, but this is because it is part of the first line standard of care for cholangiocarcinoma. This woman’s health status, or her treatment history, must somehow deviate from what Ontario Health will pay for, and so she is paying for durva infusions herself at the private clinic. And I think she must be getting clinical benefit from this because she seemed quite spry and alert (and why would she pay if it wasn’t helping), but apparently Ontario Health still won’t pay (I only overheard bits and pieces of conversation, so I don’t know the details of her condition or treatment history). This strict “recipe book” approach (the clinic manager’s phrase) limits the freedom that Canadian oncologists have regarding treatment, and means treatment is more standardized and less individualized, which, frankly, is not great once first-line treatment is over.
According to the owner, the clinic began about 20 years ago and was spurred by a conversation he had with an oncologist friend who said he was regularly sending patients to be treated in the USA because the drugs they needed weren’t available in Canada. I don’t know how payment was handled back then (some Canadian provinces have a history of paying for life-saving treatment elsewhere if it isn’t available in Canada, but have stepped back from this), but at the very least this oncologist’s patients faced the burden and expense of travelling for treatment. So, the clinic manager asked if it would benefit oncologists and patients if a private clinic was available that would handle sourcing the drugs and hire medical staff to do the infusions. The oncologist was enthusiastic about this possibility and said he couldn’t join as a partner (conflict of interest), but would certainly let his fellow oncologists know about it if it came into being. And thus a private clinic was born. Apparently it faced a great deal of media and public scrutiny when it opened because it seemed to fly in the face of Canada’s policy of socialized medicine, thus potentially creating a kind of two-tier system, but was also fully booked out for months when it opened because there were so many cancer patients in need of drugs that weren’t available in Canada. And on the one hand it isn’t a two-tier system because the clinic does not provide services that are provided by the public cancer hospital, but in a way is a two-tier system because if you can afford to pay for a treatment that isn’t formally approved in Canada (or can get the drug manufacturer to donate it) and have a referral from your oncologist, as well as approval through Health Canada’s special access program, the clinic will do its best to get you the drug and provide it to you. So, many things need to be in place to receive service from the clinic, but being able to pay is a key factor.
At present, it seemed to me, the clinic’s fortunes have faded somewhat compared to its early days. It is only open for infusions one afternoon per week, which indicates less demand, which would suggest that more drugs are now approved, available, and paid for in Ontario, and so patients receive them at cancer hospitals. My hunch is that 20 years ago many of the clinic patients were breast and lung cancer patients, and the second and third line drugs for those cancers are now much more easily and quickly approved and paid for by the government because these are much more prevalent cancers with much more patient need and demand. So these patients who once would have received treatments at the clinic now get their treatments in the cancer hospital. What’s left are patients like me — patients with extremely rare cancers whose targeted therapies aren’t even reviewed by Canada, let alone approved, because there is so little demand for them. (To be blunt, who really cares if one cholangiocarcinoma patient in Canada dies because she couldn’t get the targeted therapy she needed? Or, more quantitatively, the juice isn’t worth the squeeze because so few people are impacted. Or some other mixed metaphor about it not making budgetary sense.)
The more quickly second and third line cancer drugs are approved in Canada (and Ontario), the less need there is for this clinic, so, in a way, its apparently fading fortunes are a good thing. Though thank goodness for me that it does exist. And let me list some of the treatments that are approved and paid for by insurance in the US for cholangiocarcinoma that aren’t available and/or aren’t paid for in Canada: Keytruda (a standard second line immunotherapy in the US that is actually approved by Health Canada for some cancers, but not paid for by all provincial health plans. The role that provinces play in this is huge – Health Canada can approve drugs and negotiate prices with manufacturers, but whether provinces will pay for them is another question entirely), zenocutuzumab and at least a few other targeted therapies, Y90 radiation therapy, histotripsy, and hepatic arterial infusion pump. And these are just the ones I know about because I’ve attended webinars about them. US patients in the FB groups I belong to regularly mention treatments I know nothing about. I suppose fairer comparisons would be with the UK or Australia or France or pretty much any other wealthy country that has a national health care system. I think many of the above treatments are not available in those countries either. But, I’ll admit it’s hard being from the US, and living just a couple hours from the border, and knowing about treatments I could get there, but can’t get here.
Ok, enough about all that. I’ve grumbled about this before. Another interesting thing about this clinic is that it is very small and only accommodates 7 or 8 patients at any one time. I was the first to arrive and the last to leave because my infusion took about 5 hours. In fact, they opened the clinic a little early just to make sure they would have the time necessary for my infusion. The 2 or 3 nurses are coming right from their shifts at the cancer hospital, and so can only be there by late afternoon. In my case this meant that we didn’t get started until almost 4pm and didn’t leave until 9pm (but the next infusion should be faster because I didn’t have any allergic reactions to the first one). Unlike the cancer hospital, the space is so small that they don’t normally allow patients to have caregivers with them. They made an exception for me because my infusion was so long and my situation is pretty unusual. So my husband was there, but we didn’t really talk because it would have been too annoying to the other patients who would have heard every word. By the end of the night it was just me, my husband, the clinic owner, and two nurses watching the Blue Jays game against the Brewers on the big flatscreen TV while we all waited for the Zeno to finish dripping into my arm.
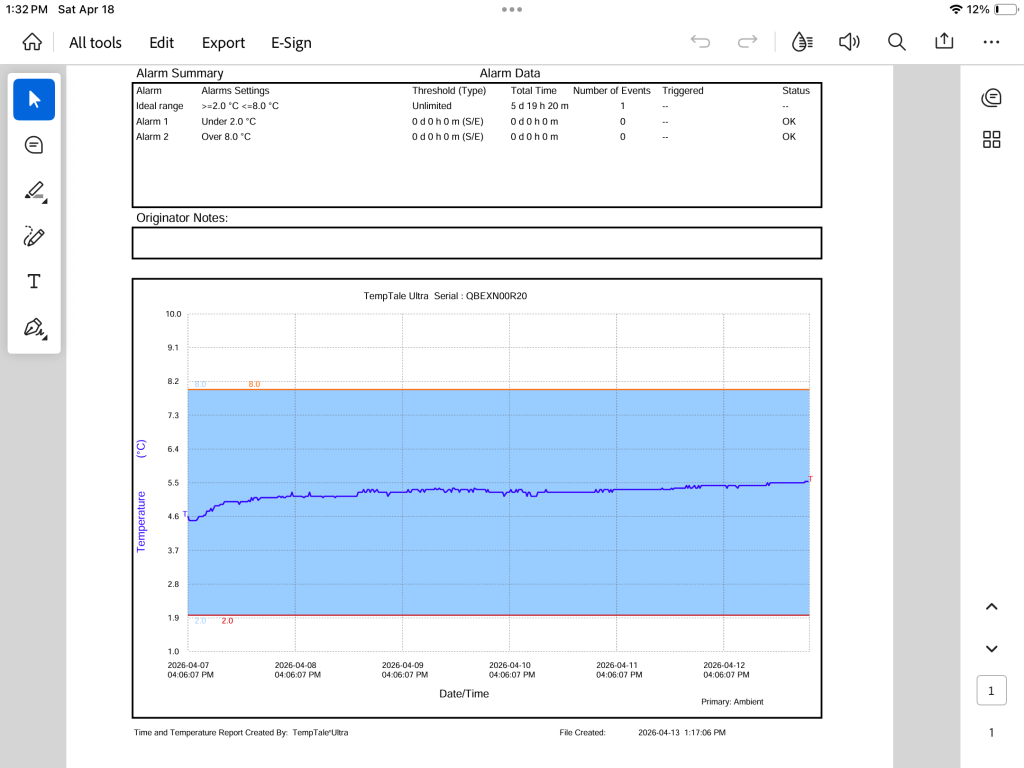
The final interesting thing about getting my infusions at this clinic is that I feel much closer to the inner workings of the process. The clinic owner informed me that there had been some drama about getting the Zeno across the border, and then, at another point, there seemed to be some confusion about where the Zeno should be sent, which was to the cancer hospital because they are open all the time, or at least there is someone available all the time to accept pharmaceuticals. The private clinic, in contrast, is on the 15th floor of a big building that houses a bunch of different businesses, and his little clinic definitely does not have someone there 24/7 to accept cancer drugs that need to be kept at a particular temperature. As he told me this I visualized a delivery person dropping off my very expensive Zeno in the building’s lobby, protected only by a quickly melting ice pack. He said it took an email to the drug distributor’s CEO to get things back on track, and there were guarantees that such confusions would not happen again. In the end, the cold chain for the Zeno was maintained (meaning it was kept within 2 – 8 degrees Celsius throughout its journey), it was delivered to the cancer hospital, and he picked it up there and brought it to the clinic the morning of my infusion. It turns out the distributor attaches an automated temperature monitor to the drug, which reports to the sender and receiver whether there are any problems with the cold chain (he sent me the report showing me the temperature of the drug as it travelled). I am very glad he spared me the story of the Zeno’s tumultuous journey until it was all in my body.
And now we wait. We are committed to paying for 4 doses (one infusion every 2 weeks). The literature about Zeno says that the median time to seeing results is 1.9 months, so I hope we’ll know (from a CT scan) by the end of May or early June whether the tumour is shrinking. Fingers crossed, everyone. I’ve become used to living (I’ve been feeling so well recently it’s hard not to), and I’d like to keep it up.

Leave a reply to Wynne Maggi Cancel reply